Heart attacks and cardiac arrests (Part 2)
Cardiac Arrest
In the last post, we defined cardiac arrest as the sudden, unexpected collapse of the heart’s mechanical pumping action that is potentially reversible. In this post, we’ll look at some of the causes of cardiac arrest, what types of cardiac arrest benefit from the use of a defibrillator, and the principles of resuscitation. In the next post, I’ll take you through the mechanics of how to perform cardiopulmonary resuscitation CPR if you are unlucky enough to be in the immediate vicinity when somebody nearby croaks it. In the one after that, we’ll consider circumstances in which CPR may be inappropriate and the application of Do Not Attempt CardioPulmonary Resuscitation (DNACPR) orders.
What happens immediately after a cardiac arrest (if you do nothing)?
The consequences of cardiac arrest are as predictable as they are dramatic. Arterial blood pressure plummets rapidly to zero, and forward blood flow through the circulation grinds to a halt. Our brains normally receive 750ml/min of oxygenated blood, which equates to fully 15% of the entire cardiac output of 5L/min, even though the brain accounts for only 2% of total body weight. This is true whether you’re concentrating hard during an exam, daydreaming, sleeping or even reading The Sun. Unfortunately, our brains have essentially zero capacity to store oxygen, and consciousness is lost within seconds of cerebral blood flow ceasing.
The clock starts ticking immediately as brain cells suffer the consequences of oxygen deprivation. One of the first vital neuronal centres to throw in the towel is the respiratory centre, located in the brainstem. Breathing stops soon after the heart stops, although the victim may take irregular gasps, known as agonal breathing, for a minute or two. I should add that some cardiac arrests are caused by somebody stopping breathing first – a heroin overdose, for example.
If the heart is not restarted and the circulation is not restored within three or four minutes, irreversible brain damage occurs. If the heart does eventually get going again after this time, the victim will suffer from permanent brain injury. The severity of such brain injury depends largely on the duration of the downtime (see later). The signs may be relatively subtle after a short downtime – forgetfulness, difficulty concentrating and personality changes. At the other extreme, permanent, catastrophic, global cerebral dysfunction, characterised by the complete absence of conscious thought, intellectual function and even self-awareness, is the end result. Although a person suffering such severe brain damage can breathe for themselves unaided, open their eyes, digest their food, exhibit sleep-awake cycles and make simple reflex responses such as blinking in response to a loud noise, they are incapable of the higher cerebral function that made them the unique person they once were. This condition used to be called a Persistent Vegetative State (PVS), although other terms such as Post-Coma Unresponsiveness (PCU) are now preferred. PCU is often confused with being brain dead, but the two conditions are entirely different, as we shall see in a later post.
Just to clarify what we mean by the downtime, there are, in fact, two downtimes. The first is the length of time from the onset of cardiac arrest to the delivery of effective CPR. During this period, there is zero blood flow in the circulation (including the brain). The second is the time from the onset of CPR to the restoration of a spontaneous circulation. During this period, there is low blood flow in the circulation (including the brain). Even with optimally performed external chest compressions, it is only about a third of normal during cardiac arrest.
Why has the heart stopped pumping?
All cardiac arrests are equal (you are technically dead, regardless), but some cardiac arrests are more equal than others (have better odds of successful resuscitation).
While it’s never a good idea to be on the receiving end of any flavour of cardiac arrest, it does pay to go down with some types rather than others if you want the best chance of springing back to life. In descending order of resurrection potential, the three types of cardiac arrest, based on the presenting ECG heart rhythm, are: 1. Shockable ECG rhythms. 2. Pulseless Electrical Activity (PEA). 3. Asystole.
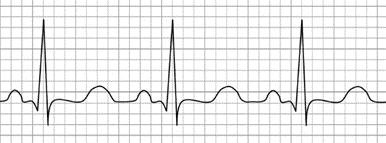
Before we discuss abnormal ECGs, it would be useful to know what a normal ECG looks like. Here is the typical ECG of a heart beating normally. I’ve only shown a single heartbeat to keep things simple:

Don’t worry. You aren’t going to have to learn how to interpret ECGs to understand the rest of this post. The important aspect of this ECG is the sharp upward spike. Ignore everything else. The spike can also point mainly downwards. It depends on which ECG lead you are looking at. Up or down, the sharp spike results from a coordinated wave of electrical activity passing through the left ventricle, which in turn serves as the stimulus for a coordinated muscular contraction. In the context of ECGs, sharp spikes are good news.
Shockable ECG rhythms
There are two of these, ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT). Don’t confuse VF with atrial fibrillation (AF), which is a relatively common disorder of heart rhythm as you get older. AF makes your heart beat fast and irregularly so that you may feel palpitations in your chest, but at least you’re still alive.
VF and pulseless VT are the two best cardiac arrest rhythms to drop down dead with because they are the most likely arrest rhythms to respond to treatment (defibrillation).
Ventricular Fibrillation (VF)
VF looks like this on an ECG monitor:
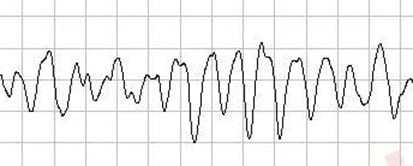
The electrical waveform is random and chaotic, which is precisely how the heart muscle is performing. Note the absence of sharp spikes. If you could observe someone’s heart in VF, it would not be entirely motionless. It would be quivering like a jelly (fibrillating, in medical parlance). It’s behaving in this way because the normal electrical signal emanating from the heart’s intrinsic physiological pacemaker that stimulates the heart muscle to contract in a regular, coordinated fashion has been replaced by a totally irregular, disorganised electrical signal. Think of a marching brass band, each member stepping forward and playing their instruments in time with each other in response to the regular beat of the big bass drum. The drummer suddenly goes bonkers, beating his drum at a ludicrously fast pace, stopping and starting in an utterly unpredictable manner. The band members are all over the place, marching this way and that as the previously beautiful rendition of the Radetsky March descends into musical chaos. That’s how the heart behaves in VF.
The treatment of VF is immediate defibrillation – with a defibrillator, of course. Simples. I’ll talk more about how to do this in the next post.
Ventricular tachycardia (VT)
VT is the other shockable cardiac arrest rhythm. It looks something like this on an ECG monitor:
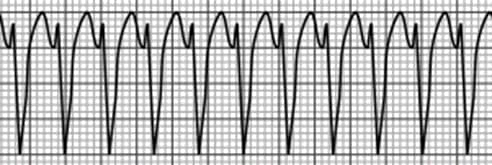
It’s very fast (the tachycardia bit) and regular, and you’ll note that this example exhibits downward spikes. If you peer a bit more closely at the spikes, though, you’ll also notice that they aren’t sharp like those of normal sinus rhythm. They are broad. So, VT is a broad-complex tachycardia.
Although VT is definitely a step up from the clusterfuck that is VF, the end result is often the same – cardiac arrest. Often, but not always. It all depends. Pulseless VT is a cardiac arrest rhythm for sure. And its shockable. However, some patients in VT do have a pulse. They are not in cardiac arrest. They might even be chatting to you casually about the fluttering in their chest. You shouldn’t be overly smug if you have this sort of VT, though, because it usually deteriorates into full-blown cardiac arrest if not quickly treated.
The treatment of pulseless VT (cardiac arrest) is exactly the same as that of VF – immediate defibrillation. (In this context, the passage of electricity through the patient’s chest is more accurately termed electrical cardioversion because the heart isn’t fibrillating. You still use a defibrillator, though.
The treatment of VT with a pulse (patient not in cardiac arrest) is more nuanced. ‘Defibrillation’ may be the best option (after you’ve anaesthetised the patient, or at least sedated them). Sometimes, it’s a better idea to try intravenous drugs first.
The commonest cause of VF and VT cardiac arrests is oxygen starvation of heart cells after the coronary artery supplying blood to them becomes acutely blocked during a heart attack. Doctors talk of the heart being irritable, which I think is a bit of an understatement. Other causes are cardiomyopathy, accidental mains electrocution, severely deranged blood electrolytes and hyperstimulation of the heart by illicit drugs such as amphetamines and cocaine.
Pulseless Electrical Activity (PEA)
PEA looks like this:
Or this:
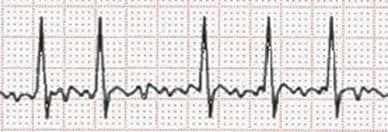
In fact, it can look like any ECG rhythm that you would normally expect to find a pulse and other signs of life. They are all characterised by the sharp spike. Just for interest, the first trace shows sinus rhythm and the second one atrial fibrillation (AF). However, to reiterate: if there is no pulse, it’s a cardiac arrest, when we call all such rhythms PEA.
The treatment of a PEA cardiac arrest DOES NOT involve the use of a defibrillator (despite what you may have seen in TV medical dramas). I’ll repeat that – you do not defibrillate a cardiac arrest victim if the heart rhythm is PEA. It will not work. Worse than that, you may induce VF in the victim’s heart. And it’s never a good idea to aimlessly wield potentially lethal electricity if there is zero benefit to be gained. It’s considered poor form to accidentally electrocute another member of the cardiac arrest team, thereby doubling the number of people in cardiac arrest at a stroke.
So, how do you treat a PEA cardiac arrest? You treat the (hopefully reversible) cause. More about this to follow.
Asystole
This is what asystole looks like on an ECG monitor:
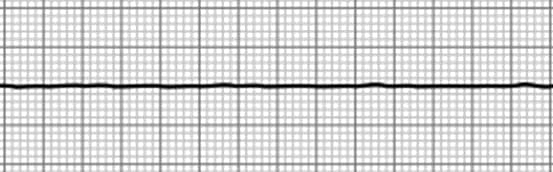
It’s a more or less horizontal, slightly undulated, flat line, signifying the absence of any electrical activity in the heart. Nada. Zilch. It is usually an indication that the heart has suffered so badly from prolonged oxygen starvation after a long downtime that it’s thrown in the towel. Unless there are special circumstances, the heart is beyond recovery. Attempting to resuscitate an asystolic heart is a waste of everybody’s time and an undignified way to go.
I said earlier not to worry if you don’t know how to interpret ECGs. I knew many doctors who didn’t have a clue, either – most of them orthopaedic surgeons. All you need to know about ECGs in the context of a cardiac arrest is that there are three, and only three, heart rhythms to recognise and deal with:
1. Shockable rhythms (VF and VT) – defibrillate.
2. PEA – treat the cause.
3. Asystole – put the kettle on.
The even better news is that you don’t even need to know that much if you ever find yourself in a situation where you are resuscitating a victim of an out-of-hospital cardiac arrest. As we will see in the next post, if you have access to an automatic external defibrillator (AED), it will diagnose the rhythm and instruct you to defibrillate only if your patient is in VF or VT. Otherwise, it will simply tell you to hold the fort (continue chest compressions) until the cavalry arrives (probably in an ambulance rather than on horseback).
How to treat PEA
The chances of successfully resuscitating somebody who has arrested in PEA are less than those of somebody in VF or VT, but much better than those of somebody in asystole. The outcome depends on the exact cause of the cardiac arrest and its reversibility (how amenable it is to targeted treatment), as well as on early identification and appropriate treatment. If you can’t identify and treat the cause, the victim’s a goner.
The eight classical causes of PEA, familiar to doctors, nurses and paramedics everywhere, are known as the 4Hs and 4Ts. The 4Hs are: hypoxia, hypovolaemia, hypothermia and hypo/hyperkalaemia (and other severe metabolic disorders). The 4Ts are: tension pneumothorax, tamponade, thromboembolic disorders and the toxic effects of drugs (prescribed or illicit).
CardioPulmonary Resuscitation (CPR)
I’m going to cover this topic in more detail in the next post. I mention it here to put defibrillation and identifying/treating the 4Hs and 4Ts into context. All the while that your patient is in cardiac arrest, they have zero cardiac output. There is no blood flow. The brain, heart and other vital organs are being starved of oxygen. While the victim themselves is technically dead, their organs aren’t. Yet. You can buy time for these organs by performing CPR – external chest compressions (+/- rescue breathing, but only if you are a trained first responder). Optimally performed chest compressions produce a blood flow of about a third of the normal resting cardiac output. That may not sound so great, but it’s better than nothing. Much, much better. It can be the difference between surviving with a good outcome and not surviving at all – or, perhaps worst of all, surviving with a poor outcome.
That’s all, folks. Although if you’re a glutton for punishment and insist on knowing more about the 4Hs and 4Ts, read on. Otherwise, you can call it a day. See you in the next post.
The 4 Hs
Hypoxia
Hypoxia is a medical condition in which the body’s organs and tissues do not receive enough oxygen to function properly. The most common causes are diseases of the lungs, such as pneumonia, COPD and acute severe asthma, or inadequate respiratory effort, for example, after taking a heroin overdose. Your two most important organs (yes, I know they’re all kinda important), your brain and your heart, happen to be the two most vulnerable to the effects of hypoxia. Whoever designed the human body got that one wrong.
The treatment of hypoxia often requires mechanical ventilation even after the successful return of a spontaneous circulation.
Hypovolaemia
Hypovolaemia is a medical condition characterised by the severe depletion of circulating blood volume. Acute major haemorrhage is an obvious cause. It may also occur in conditions where fluids and electrolytes are lost faster than they can be replaced, for example, prolonged water deprivation, severe diarrhoea, severe vomiting, and sepsis.
The treatment of hypovolaemia involves the intravenous infusion of blood, fluid and electrolytes. It’s also essential to control bleeding, even if this requires taking a critically ill/dead patient to the operating theatre.
Hypothermia
Your body’s core temperature is normally maintained at around 37ºC, even when you’re throwing snowballs at your kids on a cold winter’s day. Your fingers and toes may feel frozen, but your vital organs, nestled deep down under protective layers of skin, connective tissues, bone, and fat, remain warm and toasty. Things have gone badly wrong if your core temperature drops below 35ºC, the threshold definition of hypothermia. Perhaps you became lost in a blizzard and can’t find your way to shelter (it happens). You will feel uncomfortably cold, experiencing a deep, penetrating ache in your arms and legs. You will be shivering madly. You will become clumsy and lose coordination. Still, such mild hypothermia is hardly likely to trigger a cardiac arrest.
As your core temperature dips further, you become confused. You can’t think straight. Your speech is slurred. You feel increasingly tired and are overcome by the feeling that you really can’t be arsed (actually, that’s how I used to feel on most days until I retired). Your heart rate tends to slow gradually as your body cools, until it grinds to a halt as severe hypothermia sets in at a core temperature below 30ºC. Alternatively, your heart might take matters into its own hands before then and decide to end it all by going into VF.
Although exposure to the elements in blizzard conditions is an obvious potential cause of severe hypothermia, you are just as likely to die of hypothermia after falling into the canal in the middle of February as you are from drowning. Or if you fall asleep, blind drunk, en route from pub to home late one night in the middle of January.
From one perspective, hypothermia is a good way to end up in cardiac arrest because brain metabolism decreases with temperature, which means much longer downtimes can be survived with a good outcome. People have been fished out of freezing water in severe hypothermic cardiac arrest more than an hour after falling through the ice and have subsequently been successfully revived with full neurological recovery. Attempts to resuscitate such victims are therefore often continued for much longer than for most other cardiac arrests.
It takes a long time for the body to warm up enough for the heart to have a chance of restarting, often several hours. This fact has given rise to the old saying in resuscitation medicine that you’re not dead until you’re warm and dead. It doesn’t apply, though, if old Mrs Jones, who hasn’t been seen for several days, is found stone cold dead in her house and rigor mortis has set in.
Hyper/hypokalaemia (high and low serum potassium) and other electrolyte disturbances.
This H is a hodgepodge of severe metabolic disturbances. I’m not going to go into any detail about them, otherwise we’d be here all day. Suffice it to say that you need to treat the metabolic abnormality. For example, if a very high serum potassium has caused cardiac arrest (as it may in a person with acute kidney failure), intravenous drugs must be given PDQ both to reduce the serum potassium level and to neutralise the toxic effect of the potassium on the heart.
The 4 Ts
Tension pneumothorax
A tension pneumothorax occurs when air accumulates in the normally empty pleural space outside and surrounding the lung, and develops such a high pressure that it compresses the heart, preventing it from pumping blood effectively. It also collapses the affected lung. A tension pneumothorax is usually caused by major chest trauma. Attempts to resuscitate the victim of a tension pneumothorax in cardiac arrest will fail unless the pneumothorax is rapidly diagnosed and decompressed. Basically, you stick a large cannula through the skin between the second and third ribs, in a line running down from the middle of the collar bone, deep enough to enter the pleural cavity and vent the high pressure. An audible hiss is what you classically hear. However, with all the noise and pandemonium going on during a regular cardiac arrest resuscitation, you’d be lucky to hear Krakatoa erupting if you were the on-call anaesthetic registrar at Jakarta General Infirmary.
Tamponade
The heart does its stuff, sitting in a bag called the pericardium, which contains a small amount of fluid that acts as a lubricant, reducing friction between the beating heart and adjacent structures. It’s cardiac WD40. Cardiac tamponade occurs when an abnormal volume of fluid accumulates within the pericardium, preventing the heart from filling and emptying normally. Being stabbed in the heart will do it, in which case the abnormal pericardial fluid is blood.
To say that diagnosing tamponade during a cardiac arrest is tricky is an understatement – unless you happen to be a whizz with ultrasound and you have a machine handy. Even then, it’s far from easy. Having a high index of suspicion for cardiac tamponade is key when a patient arrests after chest trauma. Simple if there’s a great big knife sticking out of the front of the victim’s chest when they’re wheeled into the ED, but perhaps less so after they’ve been run over by a bus and their most obvious injuries are two mangled legs.
Opening the chest (emergency thoracotomy), decompressing (opening) the pericardium and performing internal cardiac massage by squeezing the heart directly with your hand greatly improve the chance of survival. It’s a big call, messy and not for the faint-hearted, but there’s nothing to lose. The victim is already dead, after all.
Thromboembolic
There are two thromboembolic causes of cardiac arrest: coronary artery thrombosis and massive pulmonary embolism. The first is basically your common or garden heart attack. Although there’s not usually much that can be done to unblock the affected coronary artery to restore blood supply to the heart during cardiac arrest, if resuscitation is successful, the patient may be rushed to the cardiac catheter lab for a percutaneous coronary intervention (PCI), a stenting procedure of the affected artery/arteries, and/or be given an intravenous infusion of a clot-busting drug such as alteplase.
Massive pulmonary embolism occurs when a large blood clot (thrombus) that has developed in a vein in the pelvis or one of the lower limbs breaks off and is carried along the venous circulation until it lodges and gets stuck, usually in the heart, causing a more or less total obstruction to the onward flow of blood. Risk factors include cancer, pregnancy, major trauma, recovery from major surgery and prolonged immobility. Although vigorous chest compressions can sometimes mechanically break up the thrombus, acute PE is more definitively treated by administering a clot-busting drug during resuscitation.
Toxins
Toxins that may cause cardiac arrest include prescribed medications taken in overdose (sedatives, antidepressants, opioid analgesics, high blood pressure medication, etc), illicit drugs (heroin, cocaine), not-so-illicit drugs (alcohol) and allergens such as peanuts in susceptible individuals. In many situations, there isn’t a specific antidote, and good quality CPR with supportive treatment is the way forward.